
Treatment
Dosing

Medication Dosing
Research has shown Congenital Adrenal Hyperplasia to be a spectrum disease. That is, a condition that manifests itself in varying degrees: the severe form being Classical Salt-wasting CAH and the mild form being Non-classical CAH with Simple-Virilizing CAH somewhere in between. In all cases, however, CAH is caused by an adrenal insufficiency resulting in impaired production of hormones.
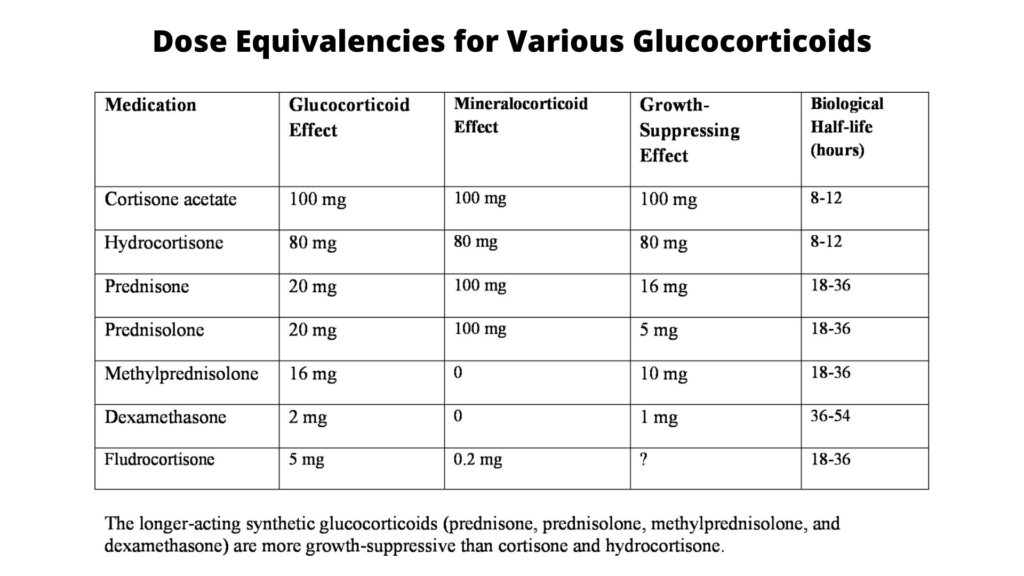
All individuals affected by Classical CAH require glucocorticoid (hydrocortisone, prednisone, dexamethasone) replacement therapy. Those with a salt-wasting component to their insufficiency also require mineralocorticoids (fludrocortisone) and sodium. The following pages outline medication dose guidelines for all individuals with CAH as agreed upon by the leading pediatric endocrinologists in the United States and Europe in 2018.
As always, this information is provided for your reference to help you better understand decisions made regarding medication dosing and in no way should be taken to be the provision or practice of medical, nursing or professional healthcare advice or services. This information should not be considered complete or exhaustive and should not be used in place of the visit, call, consultation or advice of your physician or other healthcare provider.
Dosing of Medications
Optimal Glucocorticoids Dosing. During infancy, initial reduction of markedly elevated adrenal sex hormones may require up to 25 mg hydrocortisone (HC)/m 2 .d, but typical dosing is 10-15 mg/m 2.d divided three times daily. HC oral suspension is not recommended; divided or crushed tablets of HC should be used in growing children. …HC is considered the first drug of choice. Excessive doses, especially during infancy, may causes persistent growth suppression, obesity and other Cushingoid features. Insufficient data exist to recommend higher morning or evening dosages.
Whereas HC is preferred during infancy and childhood, long-acting glucocorticoids may be an option at or near completion of linear growth. Prednisone and prednisolone need to be given twice daily.…The dose (2-4 mg/m 2.d) should be approximately one-fifth the dose of HC. The dosage of Dexamethasone is 0.25-0.375 mg/m 2.d, given once daily. Monitoring of these more potent glucocorticoids should include BP, in addition to weight, and other clinical and laboratory variables. These steroids have minimal mineralocorticoid effect, compared with HC. In children with advanced bone age, such as boys with non-salt losing CAH, initiation of therapy may precipitate central precocious puberty, requiring treatment with a GnRH agonist.
Mineralocorticoid use. All classic CAH patients should be treated with fludrocortisone at diagnosis in the newborn period. Dosage requirements in early infancy range from 0.05-0.30 mg/d, whereas typical maintenance doses are 0.05-0.2 mg/d, depending on the sodium intake.…Sodium chloride supplements are often needed in infancy at 1-3gm/d(17-51mEq/d), distributed in several feedings.
Please visit our Frequently Asked Questions page for answers to common questions related to medication dosing.
General Guidelines to Calculate Med Doses
To calculate your/your child’s doses according to the formulas set forth above, please see the web site, body surface area calculator for medications. Remember, however, that the above are just general guidelines and each patient may require variations. Ongoing monitoring of blood steroid levels is necessary. Never adjust medication doses on your own! You must consult with your doctor! This information is for your educational purposes only. Please also see section on Monitoring for CAH on this web site for more information.
Article from THE JOURNAL OF CLINICAL ENDOCRINOLOGY & METABOLISM – “Erroneous Compounding of Hydrocortisone”
The CAH Consensus Statement, 2018
We have attempted to keep all information on this web site in line with the recommendations in the “Consensus Statement on 21-Hydroxylase Deficiency” from The Endocrine Society, European Society for Paediatric Endocrinology, Societies for Pediatric Urology, and Pediatric Endocrine Society; Journal of Clinical Endocrinology and Metabolism 103(11): 1-46 November 2018. We strongly recommend that all CAH affected individuals and all parents print out a copy of the Consensus Statement and refer to it often for guidance and answers to common questions. The full text of article.

References (see below)
Congenital Adrenal Hyperplasia Due to Steroid 21-Hydroxylase Deficiency: An Endocrine Society* Clinical Practice Guideline, Phyllis W. Speiser,1,2 Wiebke Arlt,3 Richard J. Auchus,4 Laurence S. Baskin,5 Gerard S. Conway,6 Deborah P. Merke,7,8 Heino F. L. Meyer-Bahlburg,9 Walter L. Miller,5 M. Hassan Murad,10 Sharon E. Oberfield,11 and Perrin C. White12. J Clin Endocrinol Metab, November 2018, 103(11):1–46
Congenital Adrenal Hyperplasia: A Guide For Patients and Their Families, Migeon, C.; Wisniewski, A.; Gearhart, J.; Saucier, C.
Congenital Adrenal Hyperplasia, A Handbook for Parents, Gonzalez, J.; Prentice, L.; Ponder, S.;Texas Department of Health
High Frequency of Nonclassical Steroid 21-Hydroxylase Deficiency, Am. J Hum Genet 37:650-667, 1985, Speiser, P.; New, M.; et al.


CONTACT
2414 Morris Avenue, Ste 110
Union, NJ 07083
Phone: (908) 364-0272
Toll Free: (866) 227-3737
Fax: (908) 686-2019
contact@caresfoundation.org
