
Exercise
Exercise Study of Patients with Classic CAH – by Deborah P. Merke, M.D.
Why Study Exercise in Patients with CAH?
We recently discovered that patients with the most severe form of CAH (classic form) have adrenaline deficiency. Adrenaline is important in exercise and exercise naturally increases adrenaline release. We recently carried out an exercise study in patients with CAH to further explore the effects of adrenaline deficiency in patients with CAH.
Adrenaline and Congenital Adrenal Hyperplasia
We recently described that patients with the most severe form of CAH have abnormalities of the adrenal medulla, the central part of the adrenal gland (N Engl J Med 2000; 343:1362-8). Until that time, CAH due to 21-hydroxylase was known to cause abnormalities of the adrenal cortex, the outer part of the adrenal gland and was considered a disease restricted to the adrenal cortex. Cortisol, aldosterone and androgen production all occur in the adrenal cortex. The adrenal medulla secretes epinephrine, also known as adrenaline. In our previous study, patients with CAH had significantly lower adrenaline secretion (measured in 24 hour urine and in blood samples) than healthy controls. We also looked at the adrenal glands of 3 children with CAH who had an adrenalectomy. We found abnormal structure and formation of the adrenal medulla in CAH adrenals. We also found decreased storage of adrenaline hormone in the CAH adrenals compared to normal adrenal glands. Therefore, patients with CAH had decreased production of adrenaline and also had abnormal development and formation of the adrenal medulla. We are currently studying some of the practical implications of this very new finding.
Adrenaline is a stress hormone and influences many tissues. Most importantly, adrenaline plays a role in maintaining normal glucose levels, especially in young children. It also has effects on the cardiac system and influences heart rate and blood pressure. Exercise is a natural stimulus of the adrenal medulla. The goal of our exercise study was to evaluate the stress-induced adrenaline response in patients with classic CAH compared to healthy controls, and the effects of adrenaline deficiency on exercise. For this purpose we employed a standardized short-term high-intensity exercise (bicycle) test.
Our Study
Nine otherwise healthy patients with the severe or classic form of CAH (4 females, 5 males, average age 15 years) and nine healthy volunteers matched for gender, age and percent body fat participated in this study. Patients with CAH were receiving hydrocortisone and florinef and were in good clinical control. Physical activity level was derived from information on organized sports and free time activities. For example, subjects were asked how many times per week they engaged in light physical activities, such as golfing or long walks, moderate physical activities, such as hiking or bicycling, and strenuous physical activities, such as running, swimming laps or playing basketball.
Each subject underwent an exercise test to determine fitness level followed by a standardized exercise test one or two days later. The first exercise test, which measured level of fitness, was approximately 8-10 minutes and was designed to have each subject exercise to exhaustion (“Maximal Exercise Test”). The second or “Standardized Exercise Test” was approximately 20 minutes. This was a standardized high-intensity exercise test and bicycle settings were based on each subject’s level of fitness. Therefore, each participant experienced the same relative workout.

All exercise tests were performed using a cycle ergometer (bicycle) and were performed in the morning after an overnight fast (water permitted). About 60 minutes prior to each exercise test, participants drank water. CAH patients received their usual morning dose of hydrocortisone and florinef one hour before each exercise test. The healthy volunteers did not receive any medication. An intravenous catheter (IV) was placed in the arm and was used for drawing blood at predetermined time points before, during and after the exercise tests for measurements of various hormones. Subjects wore electrodes for continuous monitoring of their hearts. They also wore a fitted nose clip and mouthpiece assembly for measurement of oxygen uptake and carbon dioxide production (see Figure 1). Immediately after the end of each exercise test, subjects were questioned regarding their perceived level of effort and exhaustion.
Our Findings
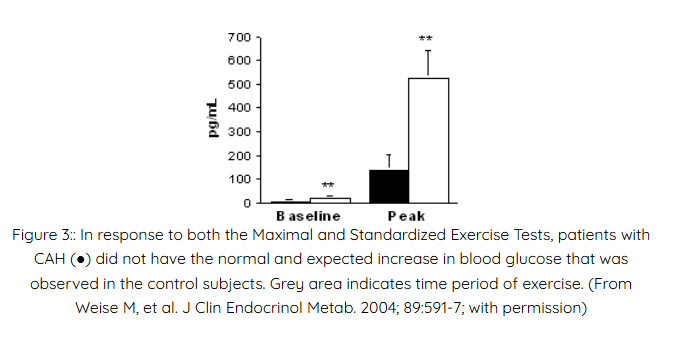
Overall, the CAH patients were slightly more physically active than the healthy controls. This was most likely due to the fact that our patients who volunteered for the exercise study tended to be very active in sports. Our patients with CAH who were not physically active, tended not to volunteer for this study. CAH patients had significantly lower adrenaline levels both at baseline (prior to exercise) and at peak exercise (when they were working the hardest) than the healthy controls (see Figure 2). Therefore, when the adrenal medulla is stimulated (by exercise), patients with CAH were not able to mount a normal increase in adrenaline levels.
We also measured other hormones which help regulate blood glucose and they did not differ between the 2 groups, with the exception of cortisol. As expected, CAH patients had different cortisol levels than the controls because CAH patients’ cortisol levels are determined by their hydrocortisone dose (their bodies are not making cortisol normally). A normal hormonal response to exercise is a rise in cortisol, but this occurs late and long after the glucose increase. Therefore, cortisol does not appear to play a major role in increasing glucose during short-term exercise. Some people
believe that extra hydrocortisone before exercise may help increase blood glucose levels or possibly affect exercise endurance. This is unknown and we are currently studying this. However, our data so far does not support using extra hydrocortisone and suggests that adrenaline has a much more important effect on blood glucose during exercise than cortisol. Unfortunately, there is no known way to replace adrenaline. We do not recommend extra hydro- cortisone for exercise. In fact, we discourage this practice because too much hydrocortisone has side effects and can be detrimental to someone’s long-term health.
None of our subjects had significantly low blood glucose during exercise or recovery. In general, children are more vulnerable to low glucose levels than adults and their body stores of glucose tend to be lower. CAH patients, particularly children with CAH, might be at increased risk of low glucose during prolonged physical stress. We currently recommend carbohydrate intake prior to prolonged exercise. We also recommend glucose containing fluids (i.e. not just water) during exercise. During illness with fever we also recommend carbohydrates (such as crackers), and glucose containing fluids, in addition to the standard “stress” doses of hydrocortisone.
Patients with CAH often love to exercise and are very active in sports. However, complaints of lack of endurance, tiring more readily than others, or just getting “wiped out” are not uncommon. It is unknown if this is due to a lack of adrenaline and/or lack of an increase in glucose. In our study, the ability to sustain exercise, the level of perceived effort, and exercise abilities were similar in both groups. Despite clearly demonstrated adrenaline deficiency, the CAH patients had normal short-term high-intensity exercise ability and tolerance, and none of our patients experienced low glucose levels. However, it remains to be determined whether adrenaline deficiency decreases endurance and ability to exercise for longer duration. This is unknown and is an area we are currently studying.
We’d like to thank the patients with CAH and the healthy controls who participated in this study!

CONTACT
2414 Morris Avenue, Ste 110
Union, NJ 07083
Phone: (908) 364-0272
Toll Free: (866) 227-3737
Fax: (908) 686-2019
contact@caresfoundation.org
